Better Graft Survival
Our technical approaches in optimizing transplanted graft survival during and after the procedure.

Why Graft Survival Matters in Hair Transplant
Each harvested follicle represents a permanent, non-renewable resource. The clinical goal is to maximize the proportion of transplanted follicles that successfully establish blood supply and produce permanent hair.
Clinical principle: A conservative approach that prioritizes graft viability supports long-term outcomes and preserves donor supply for potential future needs.
Our Graft Survival Protocols
1. Pre-Procedural Optimization
Medical assessment identifies factors that may affect healing. Patients receive guidance on optimizing their physiological state before the procedure.
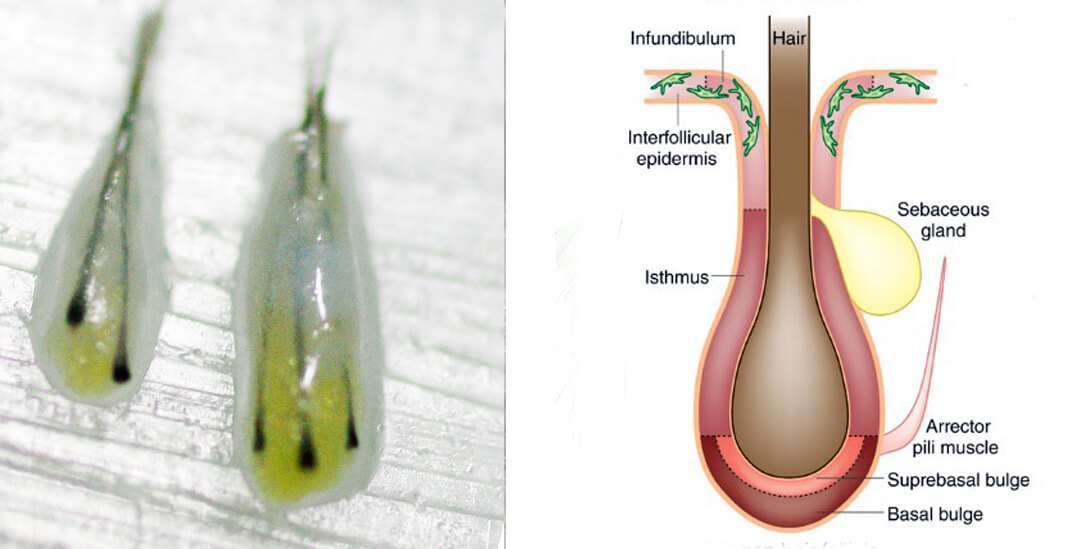
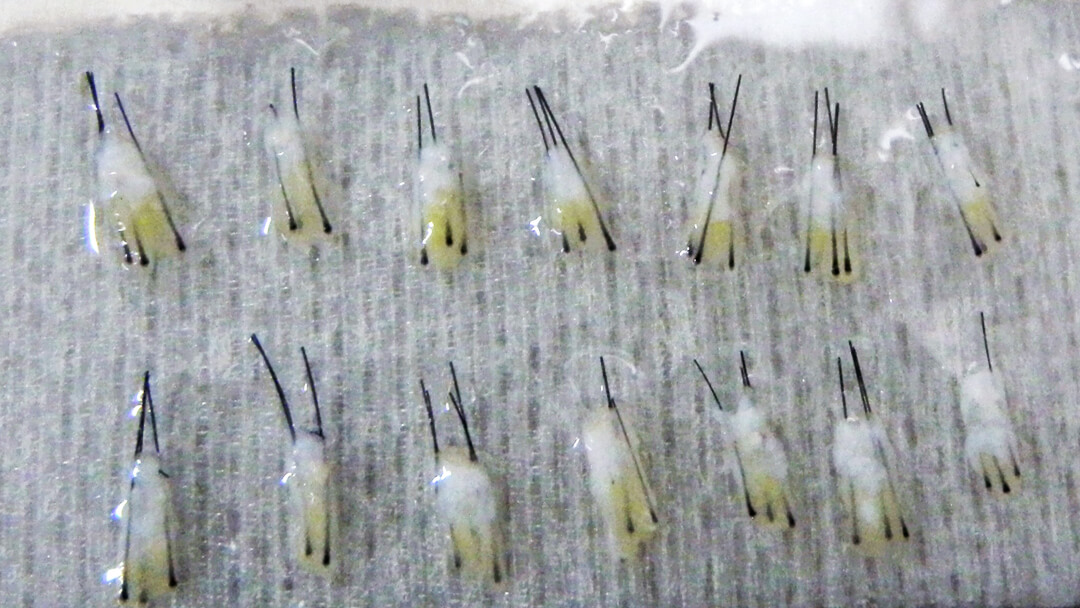
2. Gentle Harvesting Techniques
Refined instruments and careful extraction techniques help preserve follicular integrity during harvesting.
3. Physiological Storage Solutions
Grafts are placed in chilled, pH-balanced storage media that maintain cellular viability during the procedure.
4. Minimized Out-of-Body Time
Efficient team coordination reduces the time grafts remain outside the body before implantation.
5. Precise Implantation
Gentle placement techniques minimize trauma to the graft during insertion into recipient sites.
6. Post-Procedural Care
Detailed aftercare instructions support the graft during the critical revascularization phase.
Myths About Graft Survival Rates
When a clinic quotes a specific graft survival rate, it's usually marketing, not a real medical statistic. There is no reliable or ethical way to measure this for an individual patient. Rather than focusing on this unverifiable number, patients should consider the surgeon's experience, planning, and ability to design a natural result based on their unique hair.
Read More About Myths In Graft Survival Rate →Revascularization Timeline
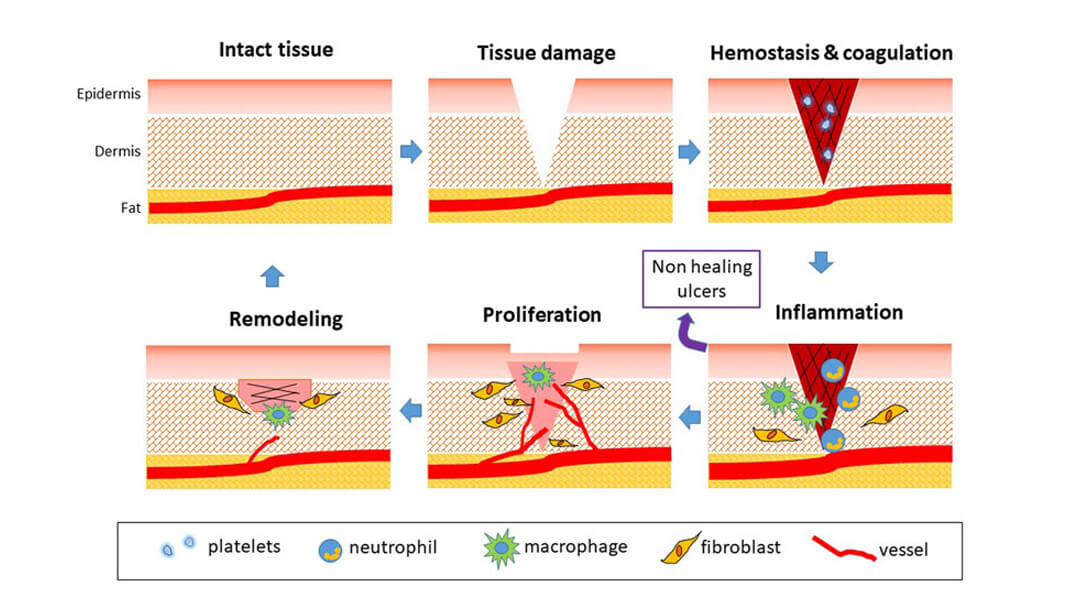
Days 1–3
Graft receives nutrients through diffusion. Gentle handling and protection are important during this phase.
Days 3–7
New blood vessels begin to form. This is the critical period for graft establishment.
Weeks 2–4
Inflammatory response subsides. Grafts become anchored in the recipient site.
Months 1–3
Follicle enters a new growth cycle. New permanent hair begins to emerge.
Key Clinical Principles
- Hydration maintenance throughout the procedure
- Controlled storage temperature (chilled, not frozen)
- pH-balanced storage media
- Reduced graft handling by multiple staff
- Minimized exposure to air
- Gentle implantation technique
- Protected healing environment post-procedure
- Scheduled follow-up monitoring
Clinical note: The combination of these protocols supports optimal graft survival. Individual outcomes vary based on patient physiology and adherence to aftercare instructions.