提升毛囊存活率
本診所在手術期間及術後優化移植毛囊存活的技術方法。

為何毛囊存活在植髮中如此重要
每個摘取的毛囊均屬永久性、不可再生的資源。臨床目標是最大化成功建立血液供應並產生永久性毛髮的移植毛囊比例。
臨床原則:優先考慮毛囊存活的保守方案,有助於長期效果,並為未來可能的需要保留捐髮區供應。
本診所的毛囊存活方案
1. 術前優化
醫學評估識別可能影響癒合的因素。患者會獲指導在手術前優化其生理狀態。
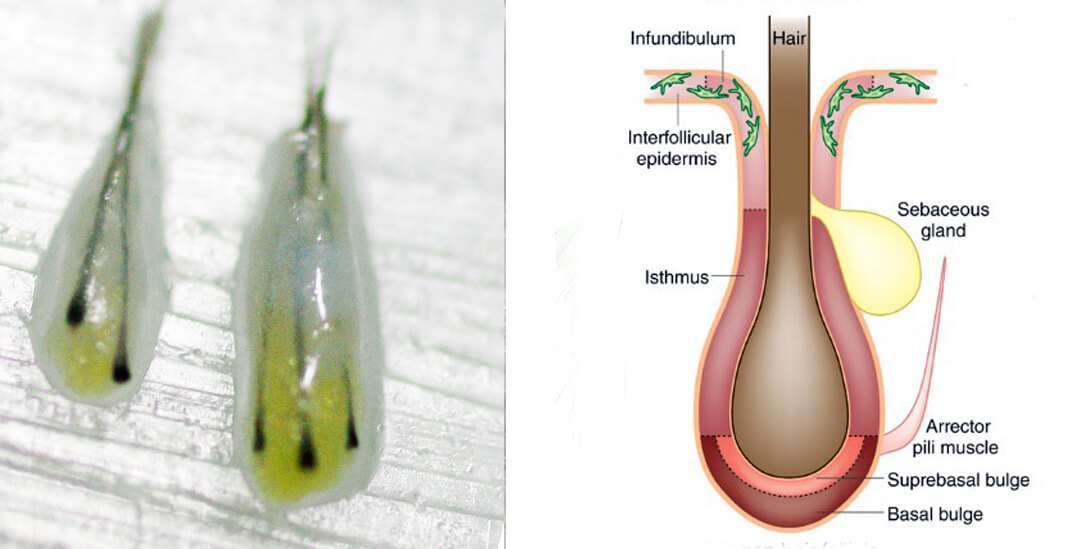
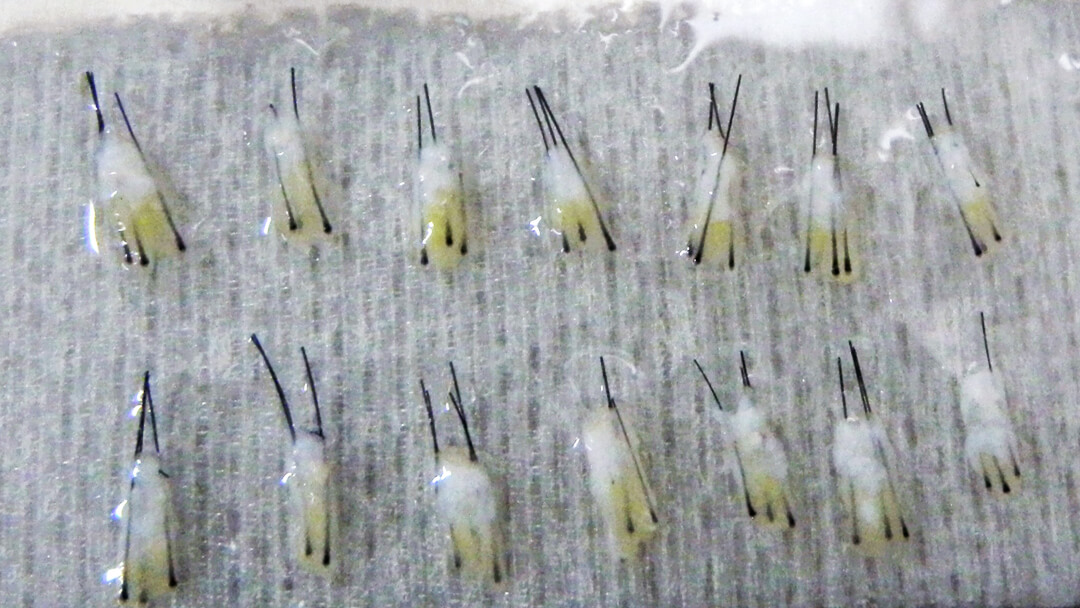
2. 輕柔摘取技術
精良的器械及仔細的摘取技術有助於在摘取過程中保護毛囊完整性。
3. 生理性儲存溶液
移植體放置於低溫、pH 平衡的儲存培養液中,在手術期間維持細胞活力。
4. 縮短體外時間
高效的團隊協調可減少移植體在植入前停留於體外的時間。
5. 精準植入
輕柔的放置技術可減少移植體在植入受區時的創傷。
6. 術後護理
詳細的術後護理指引在關鍵的血管重建階段支援移植體。
毛囊存活率的迷思
當診所引用具體的毛囊存活率時,通常是市場推廣手段,而非真正的醫學統計數據。目前沒有可靠或合乎道德的方法來為個別患者量度此數字。與其專注於這個無法驗證的數字,患者應考慮醫生的經驗、規劃,以及根據其獨特毛髮狀況設計自然效果的能力。
了解更多關於毛囊存活率的迷思 →血管重建時間表
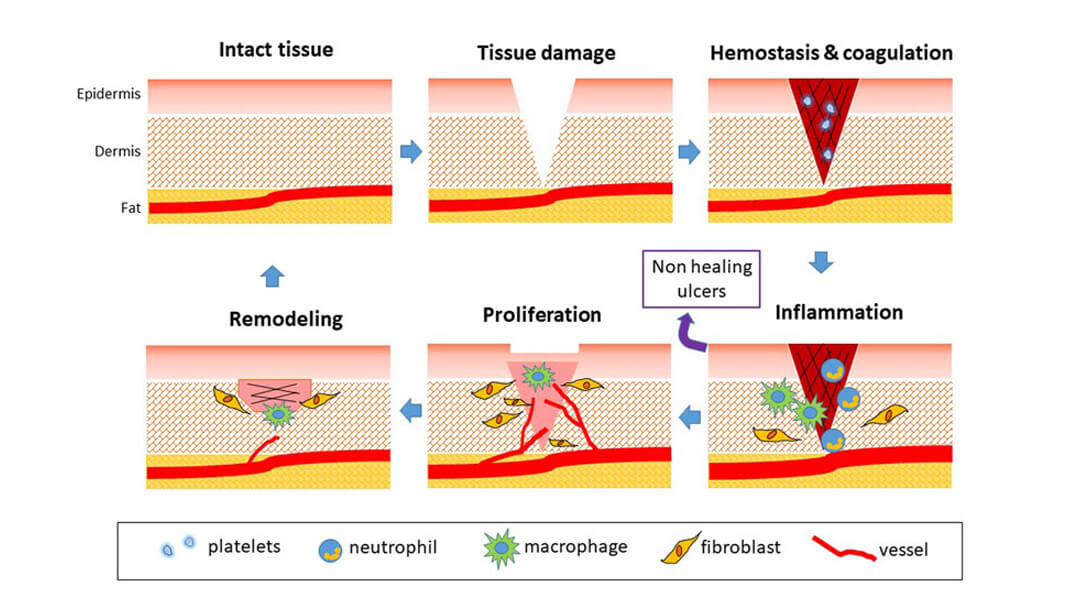
第 1 至 3 天
移植體通過擴散獲得營養。在此階段,輕柔處理及保護十分重要。
第 3 至 7 天
新血管開始形成。這是移植體建立的關鍵時期。
第 2 至 4 週
炎症反應消退。移植體固定在受區中。
第 1 至 3 個月
毛囊進入新的生長週期。新的永久性毛髮開始長出。
關鍵臨床原則
- 整個手術過程中保持移植體濕潤
- 受控儲存溫度(低溫,非冷凍)
- pH 平衡的儲存培養液
- 減少多名工作人員對移植體的接觸
- 盡量減少移植體暴露於空氣中
- 輕柔植入技術
- 術後受保護的癒合環境
- 安排覆診監察
臨床備註:這些方案的結合有助於達到最佳的毛囊存活率。治療效果因患者生理狀況及對術後護理指引的遵從程度而異。