Folliculitis Prevention Protocol
Evidence-based management of scalp inflammation to optimize healing and reduce medication risks.
What Causes Folliculitis and How Is It Classified?

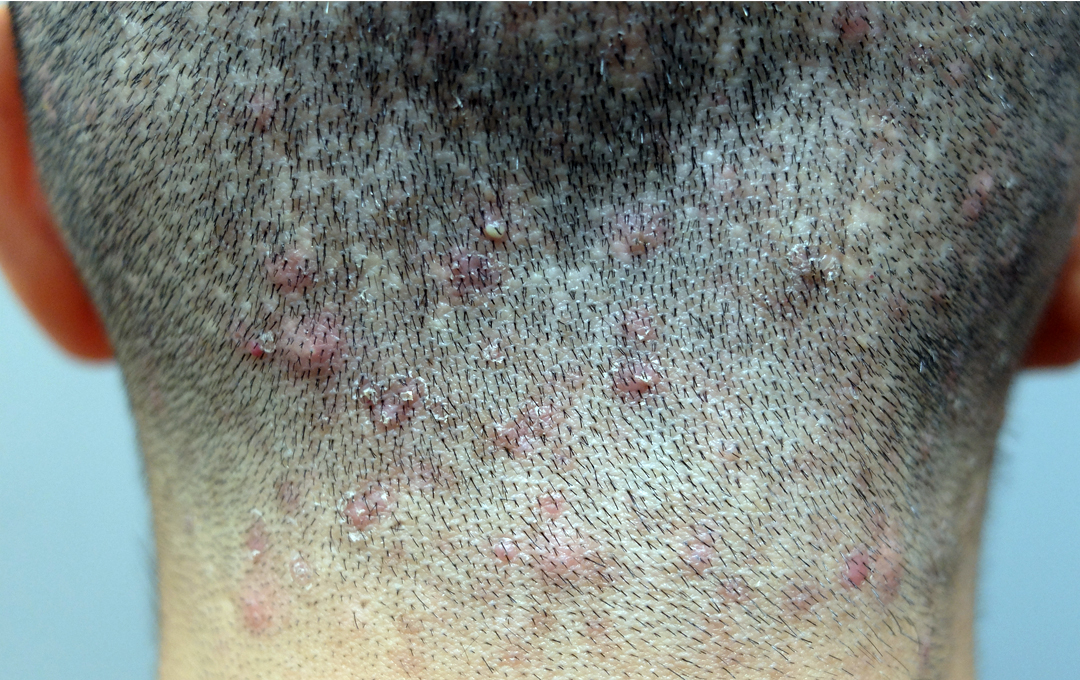
Post-operative folliculitis—small, inflamed bumps on the scalp—is a common concern. However, clinical research distinguishes three distinct types based on etiology and timing, challenging the assumption that all cases are infectious.
Three Distinct Classifications
- Early Onset (Days 1–7): Traumatic Folliculitis: An inflammatory response triggered by surgical trauma, released sebum, or buried skin fragments during graft placement. This is particularly common in patients with oily skin or pre-existing seborrheic dermatitis.
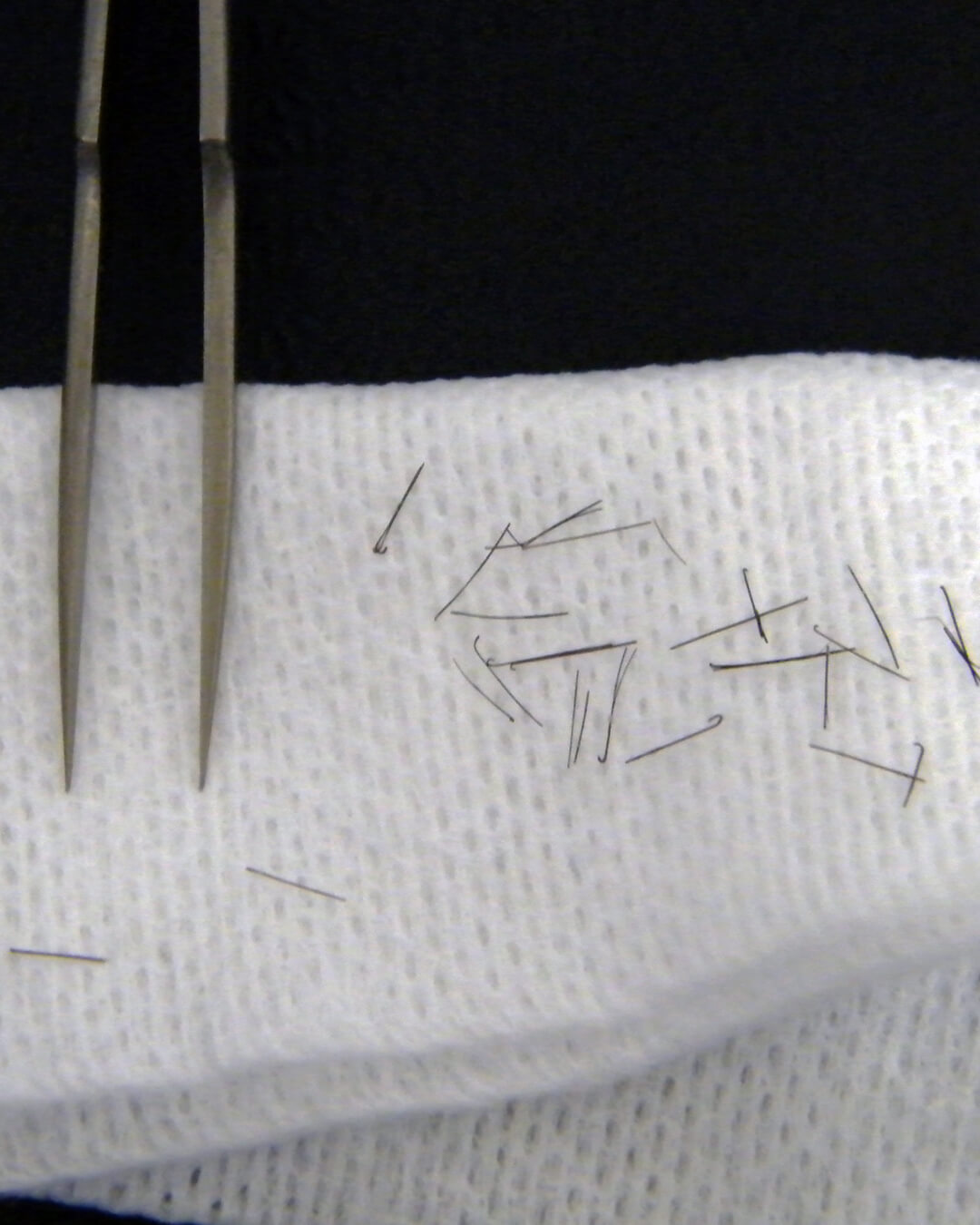
- Delayed Onset (Weeks 1–12): Foreign-Body Folliculitis: A reaction caused by dislodged hair fragments from transplanted follicles being perceived as foreign material by the immune system. This is more frequent with coarse hair types and high-density packing.
- Variable Onset: Infective Folliculitis: A true bacterial infection. This is statistically uncommon and typically occurs only with significant barrier breakdown, poor hygiene, or underlying immunocompromised conditions.
Accurate classification is essential, as the treatment for inflammatory types differs fundamentally from that of infectious ones.
How Is Folliculitis Prevented?

Effective prevention relies on a proactive, multi-layered strategy focused on minimizing inflammation rather than indiscriminately targeting bacteria.
Core Components of the Protocol
- Refined Surgical Technique: Meticulous graft preparation and precise placement are critical to reduce tissue trauma and avoid burying epithelial fragments, which are primary triggers for sterile inflammation.
- Targeted Pre-Op Preparation: For high-risk patients (e.g., those with oily skin or acne), pre-operative anti-acne medication and germ-killing shampoo might be prescribed.
- Post-Op Anti-Inflammatory Protocol: A key innovation is the administration of a short, tapering course of oral anti-Inflammatory medication immediately following surgery. This significantly suppresses the general inflammatory response and has been shown to markedly decrease folliculitis incidence.
- Antibiotic Stewardship: Routine prophylactic antibiotics are not prescribed "just in case." Evidence suggests they do not prevent inflammatory folliculitis and contribute to antibiotic resistance and unnecessary patient risk.

How Is Folliculitis Treated If It Occurs?
Management is strictly cause-specific. Misdiagnosing an inflammatory reaction as an infection can lead to ineffective treatment and delayed healing.
Tailored Interventions
- Inflammatory (Traumatic) Folliculitis: Treatment involves careful drainage of pustules, application of topical anti-inflammatory/antibiotic combinations, and continued medicated washing. Systemic antibiotics are rarely indicated.
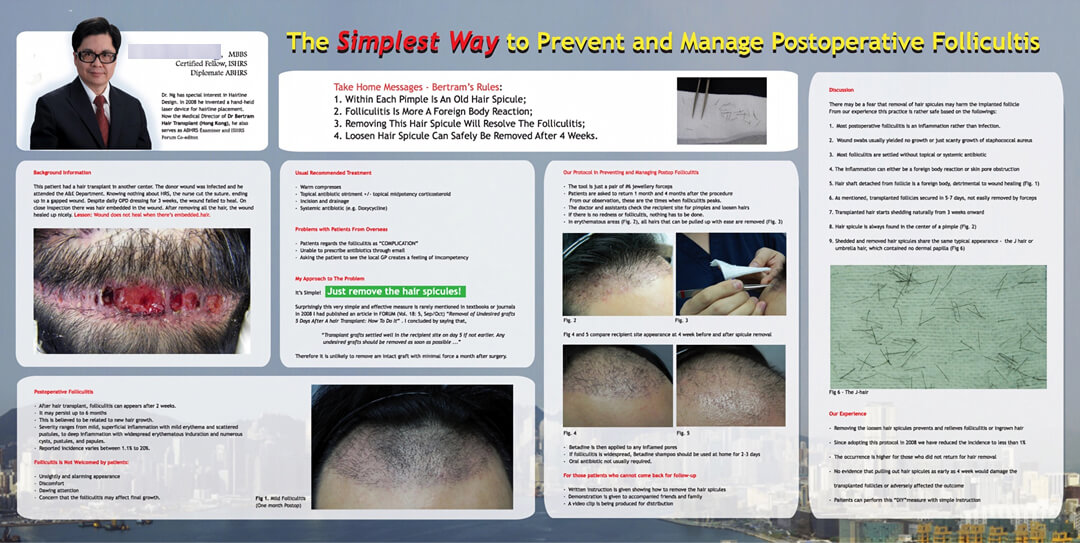
- Foreign-Body Folliculitis: The definitive treatment is the gentle removal of the embedded hair fragment using sterile tweezers. This often provides immediate relief. Topical anti-inflammatory agents support resolution.
- True Infection: Requires culture testing and targeted systemic antibiotics. Due to rigorous prevention and hygiene protocols, genuine bacterial infections are rare in modern practice.
This differentiated approach ensures faster, more comfortable resolution while minimizing drug exposure.
Inflammation vs. Infection
The distinction between sterile inflammation and bacterial infection is central to effective aftercare in hair restoration.
💡 Patient Safety
Avoiding the overuse of antibiotics spares patients from potential side effects, allergic reactions, and disruption of healthy microbiome flora.
💡 Optimized Healing
Correctly treating inflammation with anti-inflammatory measures (steroids, drainage) leads to significantly faster and more comfortable resolution than inappropriate antibiotic use.
💡 Medical Standards
This approach reflects an evidence-based, biologically accurate understanding of the healing process, moving beyond outdated "one-size-fits-all" drug prescriptions.
💡 Respect The Natural Process
Inflammation signals the body to repair. The most successful outcomes often come not from over-medicating, but from respecting the body's innate wisdom—providing it with the right conditions.
Key Principles of Inflammation Control
- Etiological Distinction: Most post-transplant bumps are sterile inflammatory reactions or foreign-body responses, not bacterial infections requiring antibiotics.
- Surgical Precision: Meticulous graft preparation and placement minimize trauma and prevent the burial of epithelial fragments that trigger inflammation.
- Targeted Prophylaxis: A short course of oral corticosteroids immediately post-op is more effective at preventing folliculitis than broad-spectrum antibiotics.
- Antibiotic Stewardship: Avoiding routine prophylactic antibiotics reduces patient risk, side effects, and the global threat of antibiotic resistance.
- Cause-Specific Treatment: Effective management requires accurate diagnosis: drainage for traumatic types, fragment removal for foreign-body reactions, and antibiotics only for confirmed infections.
Scientific References
This protocol is grounded in peer-reviewed research and clinical audits regarding recipient-site complications.
- Nusbaum B, Nusbaum A: Recipient Area Complications. In: Unger, W.P. et. Al. Hair Transplantation, Fifth Edition, informa healthcare 2011, pp 423-424.
- Marzola M, Vogel J: Complications. In: Haber R, Stough D, Hair Transplantation, Elsevier Saunders. pp 180.
- Farjo. N, Infection control and policy development in hair restoration. Hair Transplant Forum Int'l. 2008: 18(6): Jul/August. 142-144.
- Palakurthi K, Amonattana, Ng B, Pathomvanich D. A report of hospital-acquired Enterbacteria infection following hair transplant surgery. Hair Transplant Forum Int'l. 2009: 19(3): May/June. 91-93.
- Meija R. Scalp dermatology for the hair restoration surgeon: folliculitis. Hair Transplant Forum Int'l. 2008: 18(1):183.
- Ng B, Pathomvanich D, Laorwong K. Removal of undesired grafts 5 days after a hair transplant: How to do it. Hair Transplant Forum Int'l. 2008: 18(1): Sep/Oct. 180-181.
- Bunagan M: Preoperative Approach to Preexisting Scalp Lesions. In: Pathomvanich D, Imagawa K: Hair Restoration Surgery in Asians, Springer 2010, 33-36.
- Hwang S, Imagawa K: Complications and the Solutions. In: Pathomvanich D, Imagawa K: Hair Restoration Surgery in Asians, Springer 2010, 255-257.
- Shiell R: Poor Hair Growth after Hair Transplant: The X-Factor. In: Hair Transplant, Surgical and Medical, D. Stough, R. Haber. Mosby 1996, 314.